
Perhaps it’s a good sign that we’re still surprised — shocked, even — by stories like the one today about doctors at Methodist Hospital removing the wrong kidney of a patient whose other kidney was full of cancer. It suggests we have a confidence in the medical system.
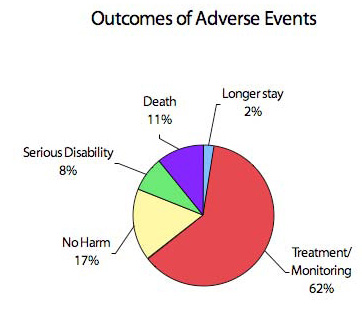 Still a study released in Minnesota two years ago found 12 deaths in the state from medical errors between October 2004 and October 2005, and 106 total medical errors in that time. A year earlier, 20 deaths were reported as a result of medical mistakes in Minnesota over a 16-month period. The most recent report found 125 errors between October 2006 and October 2007. The consequences of the mistakes are indicated in the chart .
Still a study released in Minnesota two years ago found 12 deaths in the state from medical errors between October 2004 and October 2005, and 106 total medical errors in that time. A year earlier, 20 deaths were reported as a result of medical mistakes in Minnesota over a 16-month period. The most recent report found 125 errors between October 2006 and October 2007. The consequences of the mistakes are indicated in the chart .
Not all medical mistakes are “reportable” under Minnesota law. Here are the 28 that qualify. And here is the annual report of hospitals in Minnesota and their mistake reports.
Much of the attention on the issue of medical errors came as a result of a 1999 Institute of Medicine report. “To Err Is Human: Building a Safer Health System” (pdf executive summary) set as its goal, a 50-percent reduction in medical errors by 2004.
But last October, two doctors, Tom Delbanco and Sigall K. Bell, wrote a commentary in the New England Journal of Medicine, saying that hospitals need to change the way they react to the new needs of patients after a mistake is made.
Clinicians who feel guilty after a medical error may have parallel feelings of fear — fear for their reputation, their job, their license, and their own future as well as that of their patient. Although full disclosure of medical errors is increasingly recognized as an ethical imperative, health care providers often shy away from taking personal responsibility for an error and believe they must “choose words carefully” or present a positive “spin.”2 Hospitals, insurers, and attorneys frequently advise physicians against using trigger words, such as “error,” “harm,” “negligence,” “fault,” or “mistake.” The result can be an impersonal demeanor that leads patients to view physicians as uncaring. To date, approximately 30 U.S. states have adopted “I’m sorry” laws, which to varying degrees render comments that physicians make to patients after an error inadmissible as evidence for proving liability.3,4 However, until such statutes become universal and are accepted by health care institutions, frightened clinicians are left to struggle with conflicting personal moral principles, professional ethics, and institutional policies.